
Evidence-based justification for extended rear-facing
Updated January 2022
 It’s all the rage among parents nowadays: extended rear-facing. If you’re turning your child to face forward before they’ve reached the limits of their carseat, then you’re old-schooling it and increasing your child’s risk of injury in a crash. Many pediatricians still hold onto the now ancient recommendation of turning kids forward-facing at age 1 and 20 lbs., even though their own professional organization, the American Academy of Pediatrics, hasn’t recommended that since before 2002. You were probably in grade school then.
It’s all the rage among parents nowadays: extended rear-facing. If you’re turning your child to face forward before they’ve reached the limits of their carseat, then you’re old-schooling it and increasing your child’s risk of injury in a crash. Many pediatricians still hold onto the now ancient recommendation of turning kids forward-facing at age 1 and 20 lbs., even though their own professional organization, the American Academy of Pediatrics, hasn’t recommended that since before 2002. You were probably in grade school then.
Why is it so critical for kids to stay rear-facing?
When you use the carseat right, it protects them and you from potentially being forever changed if you get into a crash.
Simple Physics Lesson
A carseat will always move toward the point of impact (Newton’s 1st Law). In a frontal collision—at 53.5%, statistically the most common type of severe/fatal crash—the entire back of a rear-facing carseat will protect the head, neck, and spine of a child as it rotates down toward the front of the vehicle. Even in a side impact, which is a more serious type of crash due to its proximity to passengers, there is usually an element of frontal movement, such as a vehicle moving forward through an intersection, as it’s hit from the side. So a rear-facing carseat will rotate down and forward, then toward the side where the impact occurs.
Click each graphic to see the motion:


Compare this to a forward-facing child in a harnessed carseat. In a frontal crash, the carseat still rotates down and forward toward the front of the vehicle, and the child will be flung forward into the harness and forward of the carseat shell. In a side impact, again the carseat rotates down and forward toward the front of the vehicle; the child comes forward into the harness and out of the carseat shell and there is rotation toward the vehicle door where the impact occurs. Because the harness is holding only the shoulders and hips, the head, arms, and legs are flung violently forward. If the harness is loose, which is one of the most common mistakes a caregiver makes, there’s a high likelihood of the child hitting the vehicle seat in front or the side pillar.
Anatomy 101
The folklore is that a child’s neck muscles aren’t developed enough to keep a baby’s neck safe in a car crash, which is why they have to face the rear of the vehicle. I suppose that’s true in a way: it does take babies time to develop their musculature so they can hold their heads up to keep their airways open. But the muscles don’t protect the fragile spinal cord, which is the bundle of nerve fibers that forms the central nervous system and is connected to the brainstem. No amount of baby push-ups will strengthen your child’s muscles to the point of protecting his spinal cord.
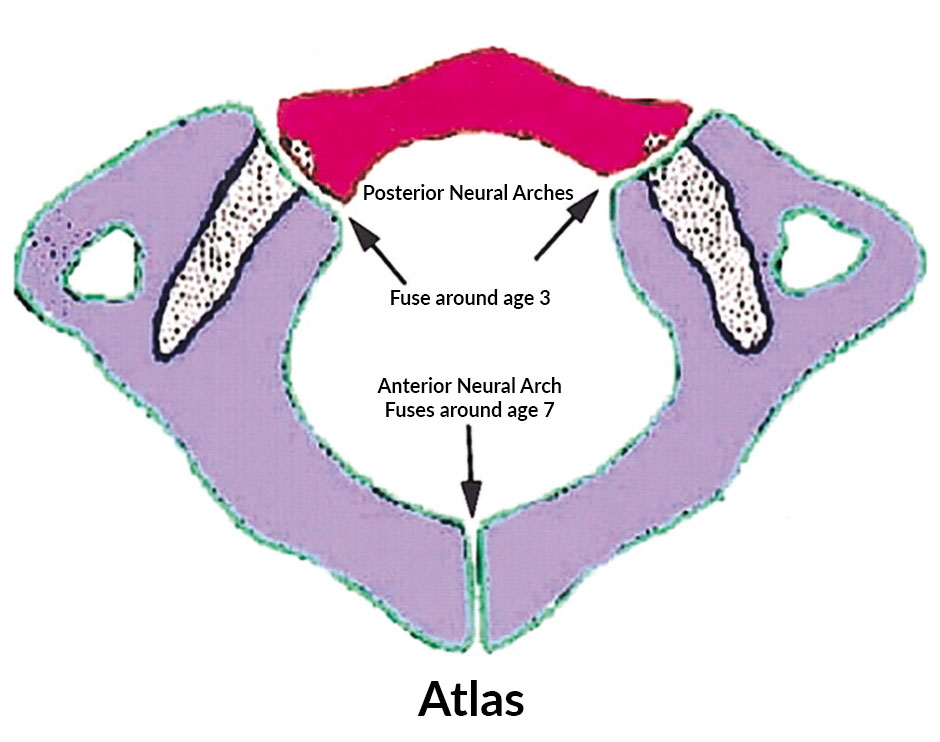
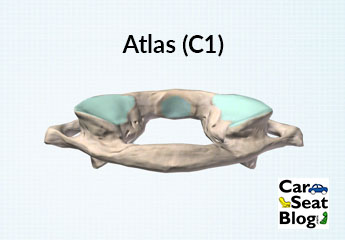
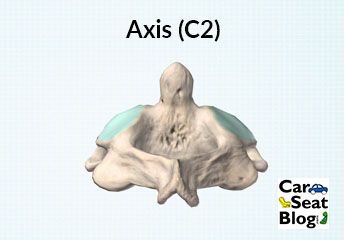
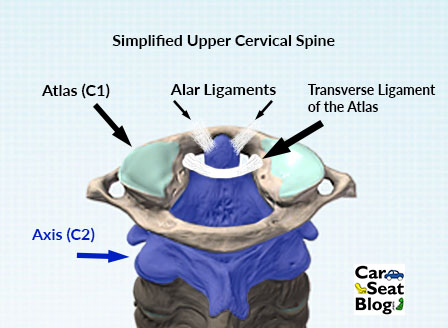
The bones of the spinal column are what actually protect the spinal cord and in infants and young children; they aren’t completely fused together for years. One of the most important cervical bones, the Atlas (C1), is what attaches the head to the spinal column. Drawings show where it ossifies, or fuses, at varying times: the anterior arch fuses around age 7, while the posterior neural arches fuse around age 3. Before it fuses, the Atlas and Axis (C2), the 2nd vertebra that the Atlas nestles into, are made of bone and cartilage, which is very pliable. These two vertebrae are held in place by ligaments, which are very elastic (lax) to allow the child to grow.
Studies of infant cadavers have shown that vertebral columns can stretch up to 2” but that the spinal cord is damaged after only ¼”. Given that a baby’s head accounts for ¼ of its total body size versus 1/7 an adult’s size, plus the immaturity of its vertebrae and laxity of the ligaments holding those vertebrae together, rear-facing seems the obvious choice.
The child’s large head shifts the fulcrum of movement—where the head swings forward—higher, elongating the spinal column and potentially causing catastrophic damage to the spinal cord. Before age 8, this fulcrum is in the upper cervical spine, at C2-C3. After age 8, the fulcrum shifts down to C5-C6, where it stays into adulthood. When you hear the term “internal decapitation,” it encompasses this movement of the upper cervical spine since the head swinging forward must happen in order for the ligaments to stretch and pull the head from the Atlas.
Another devastating injury that doesn’t show up on x-ray is called Spinal Cord Injury without Radiographic Abnormality (SCIWORA). This is when the spinal cord stretches because of the elasticity of the ligaments and cartilage in the spinal column. An x-ray will show normal bone alignment and no fractures, but the spinal cord may be irreversibly damaged. Remember that this bundle of fibers can only stretch up to ¼” before having catastrophic damage.
The evidence is clear. Rear-facing carseats protect the most fragile part of a developing child’s body: the head and spinal column. The 2018 American Academy of Pediatrics Policy Statement recommends rear-facing to the weight or height limits of the child’s carseat and instructs their pediatricians to counsel parents about rear-facing at each health visit. The National Highway Traffic Safety Administration (NHTSA) recommends rear-facing as long as possible.
Favorite Links
The American Academy of Pediatrics (AAP) has recommended since 2002 that after age 1 and 20 lbs., children should ride in a rear-facing convertible seat until reaching the weight limit of that carseat. They amended that policy in August 2018 to recommend rear-facing to the weight or height limits of the carseat.

Note how the legs fly away from the back of the vehicle seat during the rear-facing test on the left. In the forward-facing seat, the properly secured dummy bends nearly in half during the crash test. Photo courtesy Kathy Weber, ret., UMTRI, and SafetyBeltSafe USA.
2018 AAP Policy Statement on Child Passenger Safety, includes table summary of best practice recommendations and algorithm chart
2018 AAP Guidelines: rear-facing as long as possible, up to the limits of the car safety seat; includes virtually all children under 2 years of age and most children up to age 4
2018 AAP Technical Report: summary of evidence supporting best practice recommendations
The above video is a simulation comparing properly restrained 18 mo old models rear-facing to forward-facing in a 35 mph crash from the Children’s Hospital of Philadelphia Center for Research and Prevention (CIRP)
SafetyBeltSafe USA’s opinion on how long children should ride rear-facing. (How Long Should Children Ride Facing the Back of the Car?)
After reviewing studies from the U.S. and Sweden, a study published in the highly regarded British Medical Journal advises keeping children rear-facing until age 4. (www.bmj.com/cgi/content/full/338/jun11_2/b1994?view=long&pmid=19520728)
Leg injuries account for 28% of significant injuries faced by forward-facing children in crashes (Jermakian, J.S., et al. “Lower Extremity Injuries in Children Seated in Forward Facing Child Restraint Systems.” Traffic Injury Prevention 8 (2007): 171-179.)
This analysis shows how leg injuries are common among forward-facing children (Bennett, T.D., et al. “Crash Analysis of Lower Extremity Injuries in Children Restrained in Forward-facing Car Seats During Front and Rear Impacts.” Journal of TRAUMA® Injury, Infection, and Critical Care 2006;61:592-597
A tightly installed rear-facing carseat allows the vehicle and carseat to absorb crash forces and increases “ride down,” the amount of time it takes a body to come to a stop in a crash. The longer the ride down time, the less chance of injury. (http://www.car-safety.org/rearface.html)
Since there is almost always an element of forward motion in a side impact—such as when a vehicle is going straight through an intersection when it is struck on the side by a red-light runner—a rear-facing seat does a better job of keeping a child’s head contained within the safety of the seat. (http://carseatsite.com/whyrearfacing)
Evenflo is now requiring that children be age 2 before forward-facing in their convertible and combination carseats.


Approximately 75% of kids in Sweden rear-face until at least age 4. From 1999-2006, only 4 rear-facing children under age 4 were killed in crashes and their deaths were due to circumstances unrelated to the direction the carseat was facing (fire, drowning, excessive intrusion). During that same timeframe, 6 kids under age 4 facing forward in booster seats were killed; 3 of these crashes were potentially survivable crashes had the children been in rear-facing carseats. (http://www.bmj.com/cgi/content/full/338/jun11_2/b1994)
Anecdotal evidence suggests that infants around ages 10 mos.-18 mos. enter a fussy stage that makes it difficult to put them into any carseat, rear- or forward-facing. Many parents prematurely switch the rear-facing carseat forward-facing thinking that the child is objecting to riding rear-facing, when the child is objecting to being restrained at all. Visit the Car Seat Safety forums at www.car-seat.org and you’ll hear from other experienced parents regarding this phase.
The above video shows how the dummy stays contained in the seat during a rear-facing crash test. The tape on the dummy’s head is for measurement and doesn’t affect its head during the test.
This video is the companion video to the one above and shows a side view of the crash test. Note how little the head moves.
The above video shows a properly installed forward-facing seat. Note the seat belt stretch and how far forward the dummy bends.
The above video from Norway shows the differences between rear- and forward-facing carseats in an animated crash.
The above video from the Buckle Up With Brutus at The Ohio State University demonstrates the difference between rear-facing and forward-facing in crash tests.
If you need more convincing, take it from Dr. Marilyn Bull, a noted pediatrician from one of the country’s best pediatric hospitals, Riley Children’s Hospital in Indiana. This video was produced for, and used in, the current Child Passenger Safety Technician course.
Vehicle crashes are the number 1 killer of children. Protect your children to the best of your ability. Follow best practice.
Install a mirror attached to the back seat of the car itself, so the child can look at themselves in the mirror!
& optionally, give them a soft toy to play with or small book to read!
Good ideas! Just make sure that the mirror you choose is one that has soft edges and can be secured safely. There are still some mirrors sold that have hard edges.
We removed the back headrests, and our daughter was able to see more out the rear window. It also stopped her from looking out the side window and getting car sick.
Very informative article. The quote I found very similar to our situation is the parents who switch from rear-facing to front-facing due to the child objecting to being in the car seat. And to be honest, I don’t blame them. There’s nothing to see besides the chair and the view is terrible! Nor can we see our child when he’s rear-facing so if he was fussing, we wouldn’t know what was going on if both parents are seated at the front. Sounds like a niche someone should explore.
So you’re willing to let your child dictate his safety because he objects about something he can’t verbalize? Perhaps the view? Facing the rear of the vehicle means he’s looking at the front of the vehicles behind him vs. the backs of the vehicles in front of him. I think this is a narrow argument at best.
I have to agree with you Heather. This belief that it is your job as a parent to make sure (for lack of a better word) “happy” all the time. It isn’t the job of a parent to make a child happy in the car it is our job to make sure they are safe. Today’s society believes that we need to co-parent with the child instead of taking the responsibility as a parent and do what is best for them even if when they want something else. I’m not saying to not listen to your child’s concerns ,but ultimately you are the parent and even if my child objects to be rear-facing then my job is to explain to him/her that i hear them, but they will be riding rear facing. I believe in rear-facing until 4/5 or longer and booster until 12/13 because there is undeniable proof that this saves children’s lives and one of the reasons that the death rate is nearly zero in Sweden. I don’t care if they are mad. I rather them be mad at me alive then dead or seriously injured and “happy”.